8 Years Experience
MBBS, MS (Orthopaedics) FIPO (Mumbai)Consultant Paediatric Orthopaedic & Limb reconstruction surgeon.
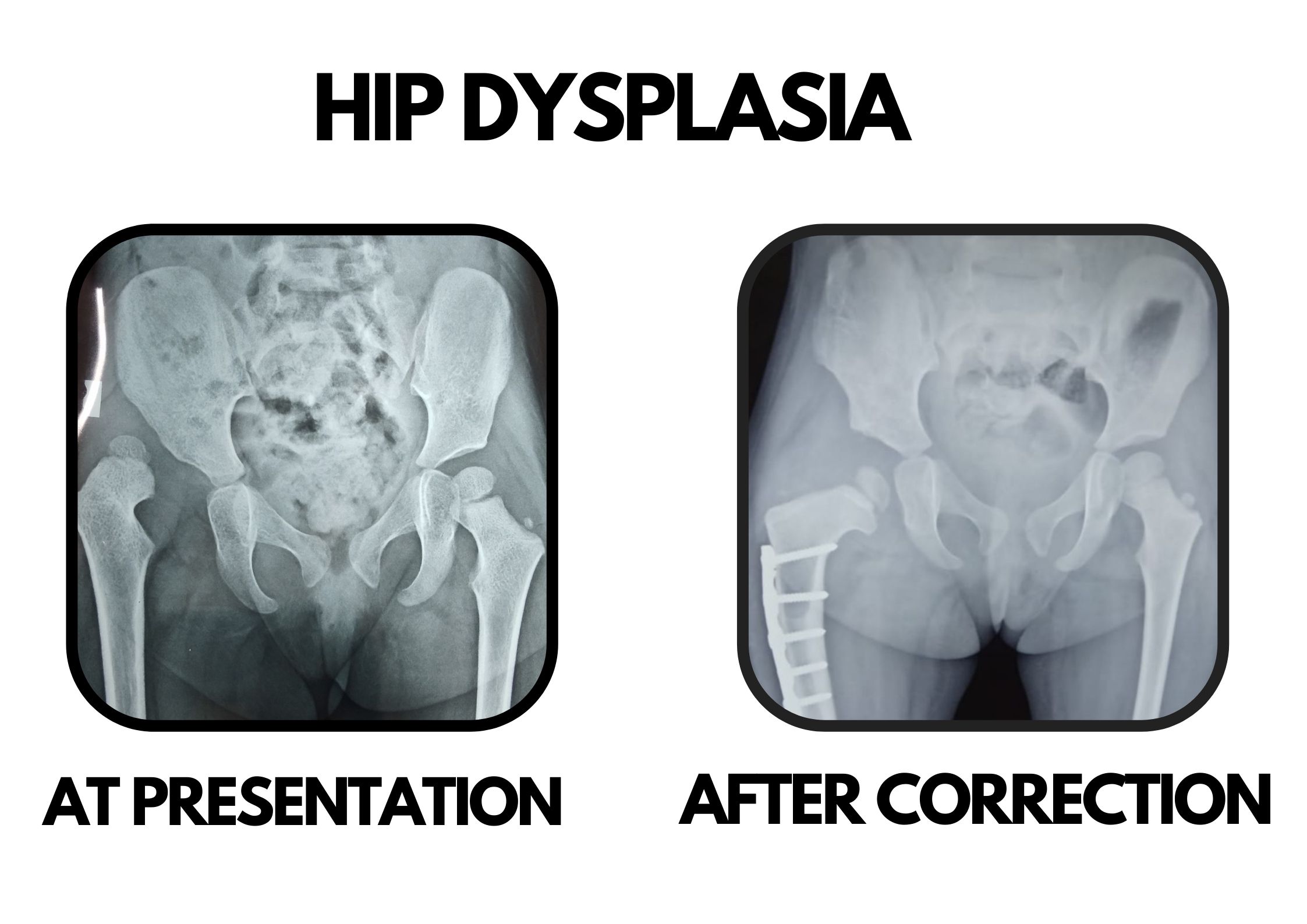
Developmental dysplasia of hip is a condition in which part of the hip joint (ball and socket joint) is dysplastic or abnormal. It is usually the socket or acetabulum part of hip joint which is usually not deep or curved enough (flat) to keep the ball (head of femur/thigh bone) concentrically reduced. Depending upon the severity, the ball can be either partially or completely out of the socket. In other cases the hip joint is reduced but is unstable and can be dislocated on clinical manueveres.
Its incidence varies between 1 to 3 in every 1000 live births. It can be present at birth or during the first year of life.It can be present in isolation or in association with other musculoskeletal disorders. It is usally more common in females, first born child, breech presentation (bottom of baby is delivered first in place of head) and in oligohydramions pregnancies.
Every child should be examined thoroughly by a paediatrician to rule out ddh and in case of any doubt, the child should be timely referred to a paediatric orthopaedic surgeon.
It is sometimes difficult to detect DDH early as there are no obvious signs present. However a careful clinical examination of both the lower limbs will be able to make out a diagnosis. Apart from examination there are other studies including USG and X-rays of the hips to confirm the diagnosis of DDH.
Treatment of DDH is age dependent:
Outcomes: Regular long term follow ups are required to ensure normal development of the hip joint. Most of children with have good functional hips after appropriate treatment. Some patients may need further surgery for residual dysplasia. However if left untreated, dysplastic hips can lead to early degeneration and pain of the affected hips.

Consultant Paediatric Orthopaedic & Limb reconstruction surgeon.
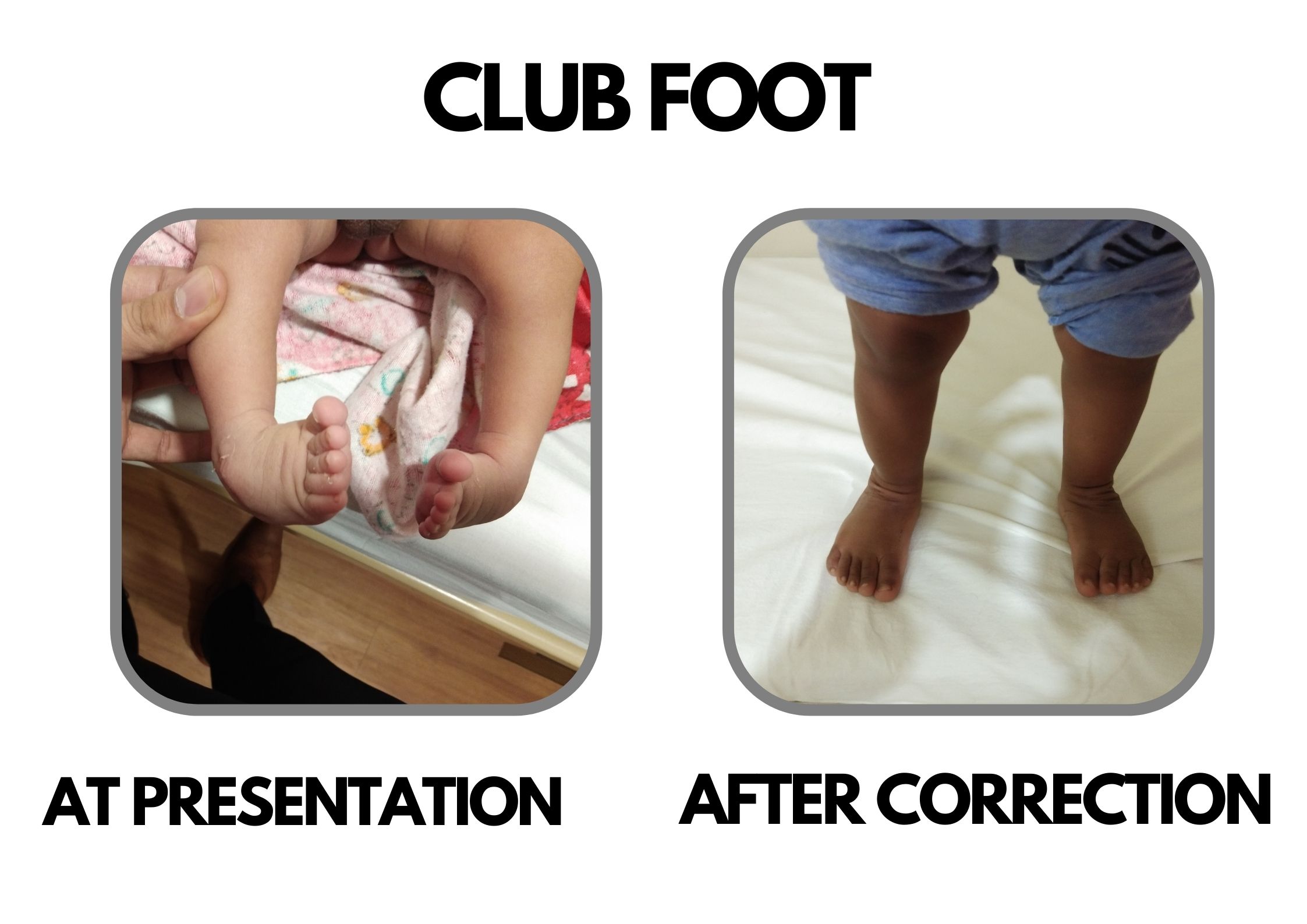
visited him as my son had CTEV (Club Foot) problem in both the feet and he advised us to get it treated at a very early age of child so treatment started in the third week since birth of the son. And it took around 2 months approx.This 2 months journey was not easy but with Dr.Deepak's treatment, advice and guidance and assurance we successfully sailed that phase.He used the best possible way to get the things done.He has exceptional command over his skills.I would highly recommend Dr. Deepak.I can't thank enough for his exceptional treatment skills, nature and being available when needed.

Dr. Deepak is one of the best experienced paediatric Orthopaedic Surgeon. My daughter met with an accident and got wrist fracture. Initially her fracture was being operated by other doctor but very disappointing as he joined the bones incorrectly and left 40% deformity. I was really upset about that then I came to know about Dr Deepak Khurana from one of my friends. He operated wrist fracture with great success. I am literally very happy that my daughter's hand is now so well and in shape. Would like to thank Dr Deepak for all his help and cooperation. Nizam (Daughter's Father)
My kid got fallen from sofa and his elbow was dislocated and I consulted him....firstly he is very friendly and he knows well how to deal with the kids. After looking after his arm he just adjust in a fraction of second and asked me to take him home and i was totally shocked and asked him what is to be done.... He just answered let him play he is fine now.... It's been 1 year my child is perfectly fine.
My son's leg was folded in L type, I showed many places but to no avail, then I got the phone number of the head and I showed my child plaster seven feet of both legs and now my baby's leg is fine. Had given it, I am wearing it. It is very important for me to be the best doctor. Thank you sir (Original) मेरे बेटे का पैर एल टाईप मे मुडा हुआ था मै कई जगह दिखाया लेकिन कोईभी फायदा नही हुआ फिर सर का फोन नम्बर मिला मै बात करके अपने बच्चे दिखाया दोनो पैरो का सात प्लास्टर कराया ओर मेरे बच्चे का पैर अब ठीक है👌 अब सिर्फ जो जुता दिया था वो पहनाता हूँ वो बहुत जरुरी है मेरे लिए सबसे बेहतरीन डॉक्टर है👌👌👌👌 thanks🙏 sir
My daughter was suffering from ligament dislocation & After several visit of different doctors I met with Dr. Deepak Khurana & he diagnosed in detail & suggest for minor surgery, Now my daughter is perfectly fine... after 10 months of operation.






Dr Deepak Khurana is a Consultant Paediatric orthopaedics & limb reconstruction Surgeon at JRSH, Jaipur. He completed his medical education from SMS Medical College. After his masters in orthopaedics, he pursued a post-doctoral fellowship in Paediatric or Read more

© Copyright 2020. All Rights Reserved | Powered by Dr Deepak khurana- Paediatric Orthopaedic Surgeon Crafted by CWM Technologies