8 Years Experience
MBBS, MS (Orthopaedics) FIPO (Mumbai)Consultant Paediatric Orthopaedic & Limb reconstruction surgeon.
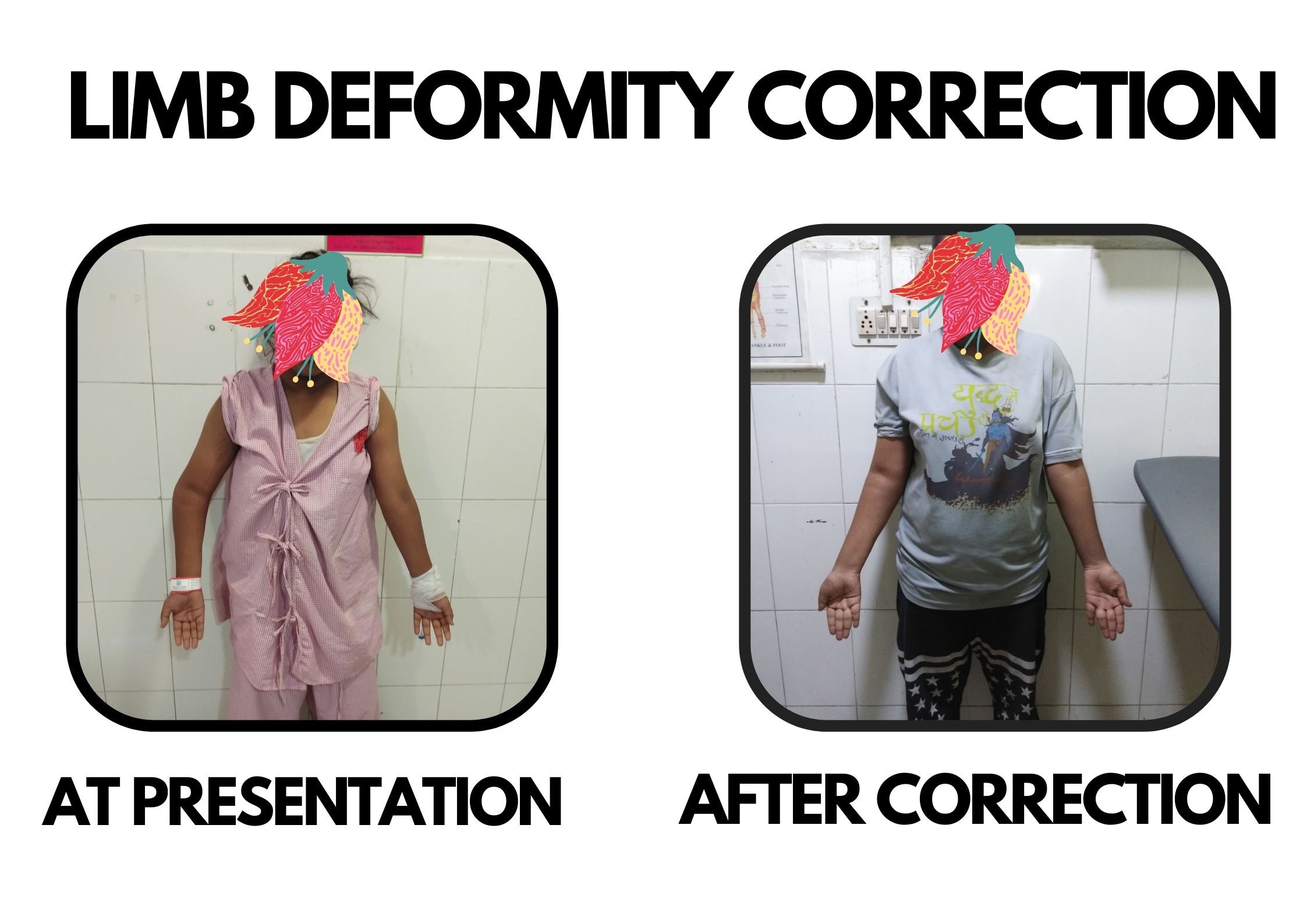
Bones may become deformed for many reasons. These include congenital (from birth), developmental (from abnormal growth during childhood), and posttraumatic (from healing in a deformed position after a fracture).
Bones may be deformed in four ways: angulation (a bend in the bone), rotation or torsion (a twist in the bone), translation or displacement (a shift in the position of the bone after a fracture or osteotomy), or limb length discrepancy (a difference in the length of a bone compared with the other side).
Although each of the different types of bone deformities can exist on its own, it is very common to see combinations of two or more of these deformity components together.
There are various aspects involved in the process of deformity correction.
Corrective osteotomy (cutting the bone) requires either internal or external fixation to stabilize the broken bone.
Internal fixation is used in cases of acute correction (corrected at once, during surgery).
External fixation is used when it is preferable or safer to correct the deformity gradually to avoid stretch injury to soft tissues, such as nerves or blood vessels. Gradual correction of deformities is similar to limb lengthening. Certain instances where external fixator has distinct advantages over other methods:
One of the newer methods for gradual correction is using the Hexapod external fixator. This new powerful correction tool can simultaneously correct all four-deformity components utilizing the six-axis correction principle. It is a computer-aided correction where the software is used to guide the correction.
In children, gradual deformity correction can also be achieved by stapling one side of the growth plate called Hemi-epihysiodesis. This stops the growth of that side while the other side of the same growth plate continues to grow. Once the bone is straight, the staple can be removed to permit symmetric growth of the entire growth plate.

Consultant Paediatric Orthopaedic & Limb reconstruction surgeon.
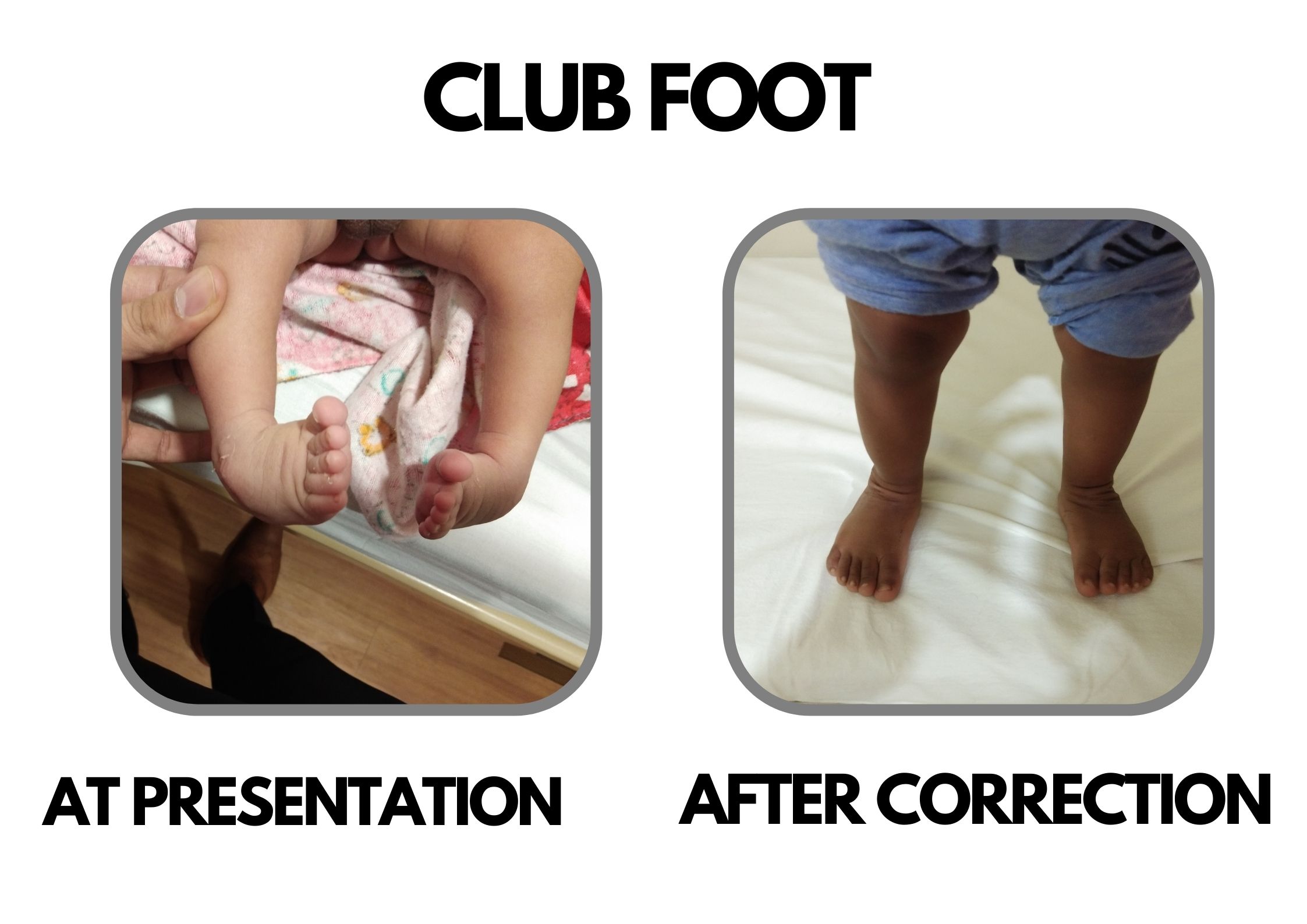
visited him as my son had CTEV (Club Foot) problem in both the feet and he advised us to get it treated at a very early age of child so treatment started in the third week since birth of the son. And it took around 2 months approx.This 2 months journey was not easy but with Dr.Deepak's treatment, advice and guidance and assurance we successfully sailed that phase.He used the best possible way to get the things done.He has exceptional command over his skills.I would highly recommend Dr. Deepak.I can't thank enough for his exceptional treatment skills, nature and being available when needed.

Dr. Deepak is one of the best experienced paediatric Orthopaedic Surgeon. My daughter met with an accident and got wrist fracture. Initially her fracture was being operated by other doctor but very disappointing as he joined the bones incorrectly and left 40% deformity. I was really upset about that then I came to know about Dr Deepak Khurana from one of my friends. He operated wrist fracture with great success. I am literally very happy that my daughter's hand is now so well and in shape. Would like to thank Dr Deepak for all his help and cooperation. Nizam (Daughter's Father)
My kid got fallen from sofa and his elbow was dislocated and I consulted him....firstly he is very friendly and he knows well how to deal with the kids. After looking after his arm he just adjust in a fraction of second and asked me to take him home and i was totally shocked and asked him what is to be done.... He just answered let him play he is fine now.... It's been 1 year my child is perfectly fine.
My son's leg was folded in L type, I showed many places but to no avail, then I got the phone number of the head and I showed my child plaster seven feet of both legs and now my baby's leg is fine. Had given it, I am wearing it. It is very important for me to be the best doctor. Thank you sir (Original) मेरे बेटे का पैर एल टाईप मे मुडा हुआ था मै कई जगह दिखाया लेकिन कोईभी फायदा नही हुआ फिर सर का फोन नम्बर मिला मै बात करके अपने बच्चे दिखाया दोनो पैरो का सात प्लास्टर कराया ओर मेरे बच्चे का पैर अब ठीक है👌 अब सिर्फ जो जुता दिया था वो पहनाता हूँ वो बहुत जरुरी है मेरे लिए सबसे बेहतरीन डॉक्टर है👌👌👌👌 thanks🙏 sir
My daughter was suffering from ligament dislocation & After several visit of different doctors I met with Dr. Deepak Khurana & he diagnosed in detail & suggest for minor surgery, Now my daughter is perfectly fine... after 10 months of operation.






Dr Deepak Khurana is a Consultant Paediatric orthopaedics & limb reconstruction Surgeon at JRSH, Jaipur. He completed his medical education from SMS Medical College. After his masters in orthopaedics, he pursued a post-doctoral fellowship in Paediatric or Read more

© Copyright 2020. All Rights Reserved | Powered by Dr Deepak khurana- Paediatric Orthopaedic Surgeon Crafted by CWM Technologies